
 Tox Talks 2025 Recap 2, Methemoglobinemia and Errors
Tox Talks 2025 Recap 2, Methemoglobinemia and Errors
Emergency Medical Minute
Contributors: Travis Barlock MD, Ian Gillman PA, Jacob Altholz MD, Jeffrey Olson MS4 In this episode, EM attending Travis Barlock and medical student Jeffrey Olson listen in to the two remaining cases presented from EMM’s recent event, Tox Talk 2025. Talk 1- Methemoglobinemia- Ian Gillman Cyanosis + chocolate-colored blood + normal PaO₂ + pulse ox stuck at ~85% = Methemoglobinemia → Treat with methylene blue The medications that can cause it can be remembered with… Watch out with methylene blue as it can cause serotonin syndrome While treating with methylene blue the...
info_outline Podcast 992: Fentanyl for Asthma
Podcast 992: Fentanyl for Asthma
Emergency Medical Minute
Contributor: Alec Coston, MD Educational Pearls: BiPAP is often effective in severe asthma, but many patients struggle with mask tolerance due to intense air hunger–driven anxiety, often compounded by hypoxia. Benzodiazepines are commonly used for anxiety, but they can depress respiratory drive, making clinical improvement difficult to interpret (a lower RR may reflect sedation rather than true physiologic improvement). Low-dose fentanyl is a useful alternative when patients cannot tolerate BiPAP despite coaching. Opioids blunt the perception of dyspnea and are well established for...
info_outline Episode 991: BRASH
Episode 991: BRASH
Emergency Medical Minute
Contributor: Aaron Lessen, MD Educational Pearls BRASH Syndrome: Bradycardia Renal Failure AV Nodal Blockade Shock Hyperkalemia Clinical Features: Profound bradycardia and shock in patients on AV nodal blockers: Commonly, Beta Blockers or Calcium Channel Blockers Etiology: Caused by an inciting kidney injury: Common triggers include precipitating illness, dehydration, or medications Results in hyperkalemia The enhanced effect of the combination of AV nodal blockade and hyperkalemia leads to a more profound presentation of shock. ...
info_outline Episode 990: Tramadol, or rather, Trama-don’t
Episode 990: Tramadol, or rather, Trama-don’t
Emergency Medical Minute
Contributor: Taylor Lynch, MD Educational Pearls: What is tramadol and how does it work? Tramadol is a Schedule IV opioid analgesic used for moderate pain and is often perceived as safer than other opioids due to lower abuse potential. It is a prodrug with weak direct μ-opioid receptor activity. The parent compound also inhibits serotonin and norepinephrine reuptake, giving it SSRI/SNRI-like properties. Tramadol is metabolized by CYP2D6 into O-desmethyltramadol (ODT), which has significantly stronger μ-opioid receptor agonism than the parent drug. What are the concerns with...
info_outline Episode 989: Young Strokes
Episode 989: Young Strokes
Emergency Medical Minute
Contributor: Aaron Lessen, MD Educational Pearls: The Case 24F brought in for anxiety. Patient is tearful, not talking, and potentially hyperventilating. History from boyfriend is that she suddenly stopped talking and started crying and it was hard to understand what she was saying. On exam, patient appears anxious and has a gaze preference for the right side and is still having difficulty speaking. Decision is made to stroke alert patient. CT shows early MCA stroke and M2 occlusion. Patient is treated by IR with mechanical thrombectomy. What are the risk factors for strokes in young...
info_outline Episode 988: Infant Botulism
Episode 988: Infant Botulism
Emergency Medical Minute
Contributor: Aaron Lessen, MD Educational Pearls: A 2025 multistate outbreak of infant botulism has been linked to ByHeart infant formula As of December 10-17th, there have been at least 51 infants with suspected or confirmed botulism who were exposed to this formula across 19 states All reported cases resulted in hospitalization but no deaths reported to date Infant botulism Occurs when C. botulinum spores germinate in the infant’s intestine, producing toxin Spores are classically found in honey but can also be in dirt or contaminated in infant formula Infants are...
info_outline Carepoint Journal Club: Trauma Discussion
Carepoint Journal Club: Trauma Discussion
Emergency Medical Minute
Carepoint Journal Club is a quarterly series with discussions about a medical topic, brought to you by Carepoint's Emergency Physicians.
info_outline Episode 987: Cough Suppressants
Episode 987: Cough Suppressants
Emergency Medical Minute
Contributor: Meghan Hurley, MD Educational Pearls: OTC Medications Dextromethorphan (DM) Most common OTC cough suppressant Minimal efficacy: Little evidence that it shortens the duration or severity of cough. Potential side effects: At recommended doses: Mild dizziness, drowsiness, GI symptoms Higher doses: Decreased consciousness, dissociative effects Guaifenesin Found in Mucinex and other severe cough/cold products Thins secretions and loosens mucus in airways No more effective than increasing oral fluid intake Prescription Medications Codeine-containing products ...
info_outline Episode 986: Lateral Canthotomy in Emergency Settings
Episode 986: Lateral Canthotomy in Emergency Settings
Emergency Medical Minute
Contributor: Taylor Lynch, MD Educational Pearls: What is orbital compartment syndrome, and how is it assessed in the emergency room? Orbital compartment syndrome (OCS) is an emergent ophthalmic condition in which intraorbital pressure in the orbital compartment rises dramatically, compromising perfusion of the optic nerve and retina, leading to risk of irreversible vision loss. OCS occurs in the context of traumatic lesions with retrobulbar hemorrhage. Intraocular pressures (IOP) are measured via tonometry as a surrogate for intraorbital pressures, with emergent pathology being present when...
info_outline Episode 985: Amiodarone vs. Lidocaine
Episode 985: Amiodarone vs. Lidocaine
Emergency Medical Minute
Contributor: Aaron Lessen, MD Educational Pearls: How do amiodarone and lidocaine work on the heart? Amiodarone Blocks potassium channels (Class III effect). Also blocks sodium and calcium channels. Additional noncompetitive beta-blocker effects. Stabilizes cardiac tissue, slows heart rate, and suppresses both atrial and ventricular arrhythmias. Lidocaine Blocks fast sodium channels in ventricular tissue (Class Ib). Shortens the action potential in ventricular myocardium, especially in ischemic tissue. Suppresses abnormal automaticity in damaged/irritable myocardium. Which one should...
info_outlineContributor: Taylor Lynch, MD
Educational Pearls:
What is Central Cord Syndrome (CCS)?
-
Incomplete spinal cord injury caused by trauma that compresses the center of the cord
-
More common in hyperextension injuries like falling and hitting the chin
-
Usually happens only in individuals with preexisting neck and spinal cord conditions like cervical spondylosis (age-related wear and tear of the cervical spine)
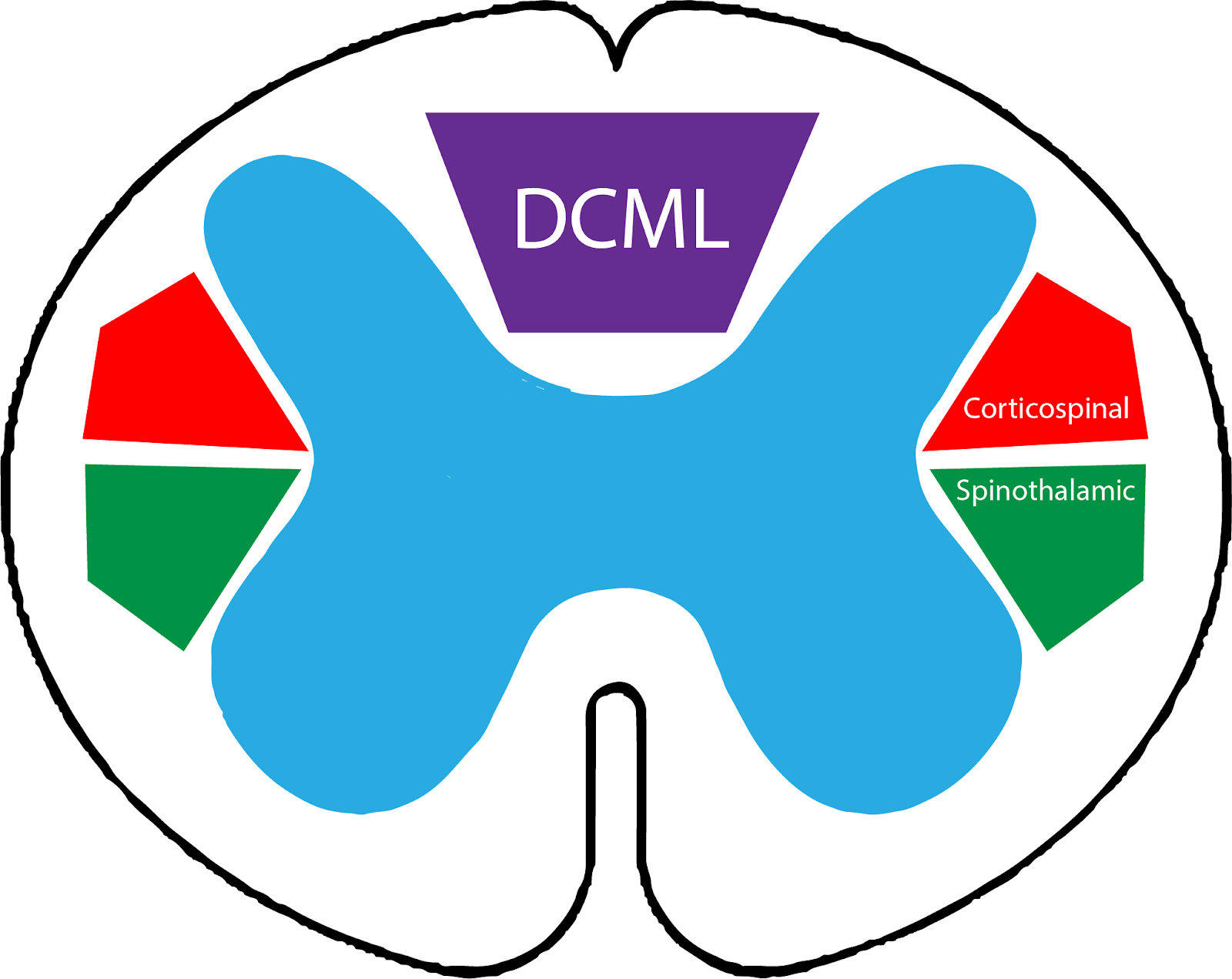
Anatomy of spinal cord
-
Motor tracts
-
The signals the brain sends for the muscles to move travel in the corticospinal tracts of the spinal cord
-
The tracts that control the upper limbs are more central than the ones that control the lower limbs
-
The tracts that control the hands are more central than the ones that control the upper arm/shoulder
-
Fine touch, vibration, and proprioception (body position) tracts
-
These sensations travel in separate tracts in the spinal cord than the sensation of pain and temperature
-
Their pathway is called the dorsal column-medial lemniscus (DCML) pathway
-
This information travels in the most posterior aspect of the spinal cord
-
Pain, crude touch, pressure, and temperature tracts
-
These sensations travel in the spinothalamic tract, which is more centrally located
-
These signals also cross one side of the body to the other within the spinal cord near the level that they enter
How does this anatomy affect the presentation of CCS?
-
Patients typically experience more pronounced weakness or paralysis in their upper extremities as compared to their lower extremities with their hands being weaker than more proximal muscle groups
-
Sensation of pain, crude touch, pressure, and temperature are much morelikely to be diminished while the sensation of fine touch, vibration, and proprioception are spared
What happens with reflexes?
-
Deep tendon reflexes become exaggerated in CCS
-
This is because the disruption in the corticospinal tract removes inhibitory control over reflex arcs
What happens to bladder control?
-
The neural signals that coordinate bladder emptying are disrupted, therefore patients can present with urinary retention and/or urge incontinence
What is a Babinski’s Sign?
-
When the sole of the foot is stimulated a normal response in adults is for the toes to flex downward (plantar flexion)
-
If there is an upper motor neuron injury like in CCS, the toes will flex upwards (dorsiflexion)
How is CCS diagnosed?
-
CCS is mostly a clinical diagnosis
-
These patient also need an MRI to see the extent of the damage which will show increased signal intensity within the central part of the spinal cord on T2-weighted images
How is CCS treated?
-
Strict c-spine precautions
-
Neurogenic shock precautions. Maintain a mean arterial pressure (MAP) of 85-90 to ensure profusion of the spinal cord
-
Levophed (norepinephrine bitartrate) and/or phenylephrine can be used to support their blood pressure to support spinal perfusion
-
Consider intubation for injuries above C5 (C3, 4, and 5 keep the diaphragm alive)
-
Consult neurosurgery for possible decompression surgery
-
Physical Therapy
References
-
Avila, M. J., & Hurlbert, R. J. (2021). Central Cord Syndrome Redefined. Neurosurgery clinics of North America, 32(3), 353–363. https://doi.org/10.1016/j.nec.2021.03.007
-
Brooks N. P. (2017). Central Cord Syndrome. Neurosurgery clinics of North America, 28(1), 41–47. https://doi.org/10.1016/j.nec.2016.08.002
-
Engel-Haber, E., Snider, B., & Kirshblum, S. (2023). Central cord syndrome definitions, variations and limitations. Spinal cord, 61(11), 579–586. https://doi.org/10.1038/s41393-023-00894-2
Summarized by Jeffrey Olson, MS3 | Edited by Jorge Chalit, OMS3
Donate: https://emergencymedicalminute.org/donate/