REBEL CAST - RENOVATE Trial: HFNC vs BPAP in Acute Respiratory Failure
Release Date: 02/05/2026
 REBEL MIND Ep7 - Growth vs Fixed Mindset in Medicine
REBEL MIND Ep7 - Growth vs Fixed Mindset in Medicine
REBEL Cast
🔑Key Points 🌱 Growth mindset transforms learning – Residents and students who believe skills can be developed are more open to feedback, more resilient after failure, and more engaged in practice. 🧠 Language matters in feedback – Simple reframes such as “You’re developing procedural skills” instead of “You’re not strong at procedures” encourage persistence and normalize the learning curve. 🤝 Mindset shapes team culture – Growth mindset leaders foster psychological safety, invite input, and create collaborative teams. Fixed...
info_outline REBEL MIND Ep6 – How to Sleep When the World Says You Can’t
REBEL MIND Ep6 – How to Sleep When the World Says You Can’t
REBEL Cast
🔑Key Points ☕ Try the coffee nap! Where you combine caffeine and a 30-minute nap to then have that boost energy and alertness by the time it kicks in. 💤 Sleep isn’t optional—it’s crucial for memory, mood regulation, and physical recovery. It is fundamentally different from rest ❌ Replacing sleep with caffeine isn’t effective and can have negative health impacts. Make getting enough sleep a priority 🌞 Sunlight exposure is important for maintaining circadian rhythms and sleep quality. This applies even if you work as a nocturnist 💡 Creating a personalized sleep...
info_outline REBEL MIND Ep5 - Applying Performance Science In and Out of the Emergency Department
REBEL MIND Ep5 - Applying Performance Science In and Out of the Emergency Department
REBEL Cast
📌 Key Points 🔍 Understanding the Why: The significance of understanding underlying causes, beyond initial diagnoses, in both sports and emergency medicine is explored. ⏱️ Recovery Focus: Emphasizing the importance of recovery time and small daily choices in optimizing performance for both athletes and emergency physicians. 📊 Data-Driven Insights: The Arena Labs approach uses personalized data, leveraging wearable technology and expert coaching to tackle burnout and enhance well-being. 🤝 Personalization and Partnership: Arena Labs’ collaboration with emergency...
info_outline REBEL Core Cast 150.0: Emergency Medicine Consults: How to Call a Consult + Handle Pushback
REBEL Core Cast 150.0: Emergency Medicine Consults: How to Call a Consult + Handle Pushback
REBEL Cast
In this episode of Rebel Core Content, Swami breaks down one of the most important (and most underrated) skills in emergency medicine: how to give a clean, effective consult—and what to do when you get pushback. Learn a simple 4-step framework to structure every consult (introduce yourself, lead with the ask, give a focused summary, and close the loop), plus ready-to-use scripts for common scenarios. We also cover how to respond to refusals, keep conversations professional, and escalate appropriately when patient safety or disposition is at risk.
info_outline REBEL CAST: The RSI Trial – Ketamine vs Etomidate in Rapid Sequence Intubation
REBEL CAST: The RSI Trial – Ketamine vs Etomidate in Rapid Sequence Intubation
REBEL Cast
REBEL Cast: The RSI Trial — Ketamine vs Etomidate in Critically Ill Adults In this episode, we break down the 2025 NEJM RSI trial comparing ketamine and etomidate for tracheal intubation in critically ill adults (Casey et al., PMID: 41369227). This multicenter randomized trial enrolled 2,365 patients across ED and ICU settings and asked a clinically important question: does ketamine improve 28-day mortality compared with etomidate? What we cover: Primary outcome: no statistically significant difference in 28-day mortality Secondary signal: higher “cardiovascular collapse” with...
info_outline REBEL CAST - RENOVATE Trial: HFNC vs BPAP in Acute Respiratory Failure
REBEL CAST - RENOVATE Trial: HFNC vs BPAP in Acute Respiratory Failure
REBEL Cast
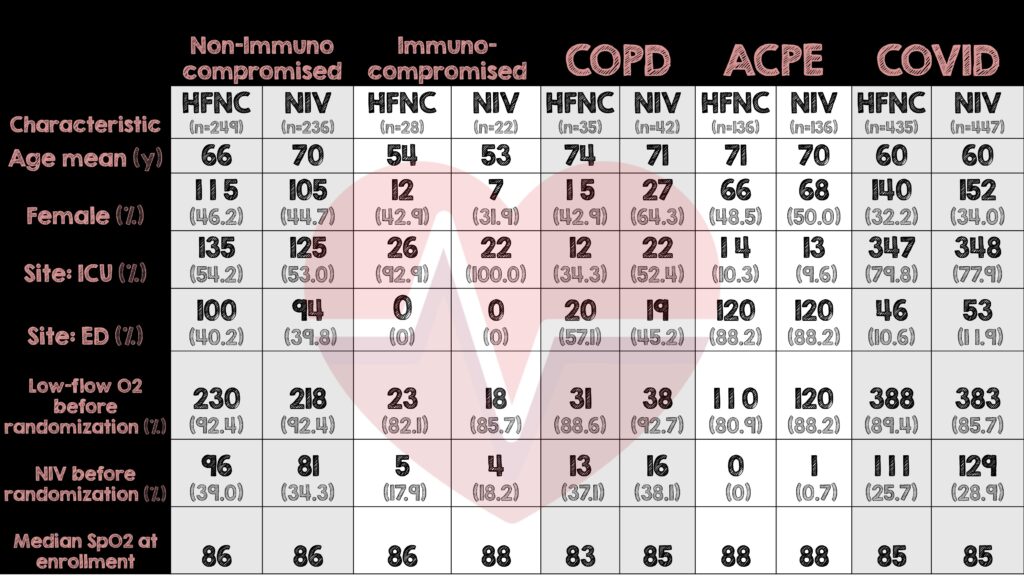
📌 Key Points 💨 HFNC met criteria for non-inferiority to BPAP for preventing intubation or death within 7 days in four of the five ARF subgroups. 🧪 Bayesian dynamic borrowing increased power across subgroups but created variable certainty, especially in smaller groups such as COPD. 🫁 The immunocompromised hypoxemia subgroup did not meet non-inferiority, leading to early trial stopping for futility. ⚖️ Rescue BPAP use, subgroup-specific exclusion criteria, and non-standardized BPAP delivery are important contextual factors that influence...
info_outline REBEL MIND Ep4 – Rest Is Not Sleep: The Seven Dimensions of True Recovery
REBEL MIND Ep4 – Rest Is Not Sleep: The Seven Dimensions of True Recovery
REBEL Cast
🗝️Key Points Rest isn’t a luxury; it’s a necessity and differs significantly from sleep in terms of mental and physical recovery needs. Uncovering the seven types of rest can highlight diverse needs: physical, mental, sensory, creative, emotional, social, and spiritual. Rest from high-stress environments such as the ED is crucial for reducing exhaustion, enhancing decision-making, and maintaining empathy. The necessity for intentional rest: tailor your rest strategies to meet personal recharge needs effectively. Rest should be deserved, not...
info_outline REBEL Core Cast 149: Review of Corticosteroids in Community-Acquired Pneumonia
REBEL Core Cast 149: Review of Corticosteroids in Community-Acquired Pneumonia
REBEL Cast
🗝️ Key Points 💉 Hydrocortisone Saves Lives: The 2023 Cape Cod Trial (NEJM) showed a clear mortality benefit and reduced need for intubation in severe CAP patients treated with hydrocortisone. 📊 Guidelines Are Catching Up: The SCCM (2024) and ERS now recommend steroids for severe CAP, while ATS/IDSA updates are still pending. 🔥 Redefining “Severe”: Patients requiring high FiO₂ (>50%), noninvasive or mechanical ventilation, or PSI >130 meet criteria for steroid therapy — even outside the ICU. 🍬 Main Risk = Hyperglycemia: Elevated glucose was the most...
info_outline REBEL CAST – IncrEMentuM26 Speaker Spotlight : Drs. Sara Crager and Ryan Ernst
REBEL CAST – IncrEMentuM26 Speaker Spotlight : Drs. Sara Crager and Ryan Ernst
REBEL Cast
📝Introduction Welcome to this special edition of the REBEL Cast, where we unravel key highlights and educational insights from the IncrEMentuM Conference in Spain. This event is a cornerstone for advancing emergency medicine education, drawing esteemed speakers and participants from around the globe. As emergency medicine gains traction in Spain, this conference has become an essential platform for knowledge exchange and professional growth. Today, host Dr. Mark Ramzy shines a spotlight on two phenomenal educators: Drs. Sara Crager and Ryan Ernst who shared their expertise and...
info_outline REBEL MIND Ep3 - Performance Coaching in Medicine
REBEL MIND Ep3 - Performance Coaching in Medicine
REBEL Cast
📌 Key Points 💪 Building Resilience: Rebel MIND, in partnership with Arena Labs, introduces a science-based performance coaching platform specifically tailored for healthcare professionals, focusing on stress management and burnout prevention. 🤝 Personal Insights: Jackie Penn shares her journey from exercise science to digital coaching, highlighting the importance of tailored coaching in high-pressure environments like healthcare. 🎯 Clinician-Centric Approach: Understanding unique challenges faced by ER doctors, the program provides practical tools for stress and transition...
info_outline-
Bilevel Positive Airway Pressure (BPAP) has long been a foundational modality in the management of acute respiratory failure (ARF), particularly in COPD exacerbations and cardiogenic pulmonary edema, where it can rapidly reduce work of breathing and improve gas exchange. It remains a core tool in our respiratory support arsenal.
-
High-flow nasal cannula (HFNC), however, has expanded what we can offer patients by delivering many of the same physiologic benefits through a far more comfortable interface. With high flows, modest PEEP, and effective dead-space washout, HFNC can improve oxygenation and decrease work of breathing while preserving the ability to talk, cough, eat, and interact with staff and family. This combination of physiologic support and tolerability makes HFNC especially attractive in patients where comfort, anxiety, or cardiovascular stability are key considerations, and in settings where prolonged noninvasive support may be needed. Rather than competing with BPAP, HFNC broadens our options in ARF and allows us to better match the modality to the patient and their underlying disease process.
-
The RENOVATE trial set out to answer a high-impact question across five distinct etiologic groups: Is HFNC non-inferior to BPAP (NIV) for preventing intubation or death in acute respiratory failure?
Is HFNC non-inferior to BPAP for rate of endotracheal intubation or death at 7 days in patients with acute respiratory failure due to a variety of causes?
- Multicenter, randomized non-inferiority trial
- 33 Brazilian hospitals
- Nov 2019 – Nov 2023
- Adaptive Bayesian hierarchical modeling with dynamic borrowing
- Open label, outcome adjudicators blinded
- Patients were classified into 5 subgroups