
 Fix 95% of SI Joint Problems in 30 Days
Fix 95% of SI Joint Problems in 30 Days
The Zac Cupples Show
Want personalized help fixing this? See if we're a fit: Want to learn the system yourself? Get 49 lessons on movement, pain, and training (free): I’m Zac Cupples, a physical therapist and movement coach with 14+ years of experience helping people move better, hurt less, and train smarter. I’ve worked in private practice, professional sports, and online coaching, including time in the NBA. My focus is simple: combine biomechanics, pain science, and strength training so people get real results. We don’t chase symptoms. We fix systems. Quick background: Earned my Doctorate of Physical...
info_outline You've Been Lied to About Posture
You've Been Lied to About Posture
The Zac Cupples Show
Want personalized help fixing this? See if we're a fit: Want to learn the system yourself? Get 49 lessons on movement, pain, and training (free): I’m Zac Cupples, a physical therapist and movement coach with 14+ years of experience helping people move better, hurt less, and train smarter. I’ve worked in private practice, professional sports, and online coaching, including time in the NBA. My focus is simple: combine biomechanics, pain science, and strength training so people get real results. We don’t chase symptoms. We fix systems. Quick background: Earned my Doctorate of Physical...
info_outline You're Doing Glute Bridges Wrong (Do THIS Instead)
You're Doing Glute Bridges Wrong (Do THIS Instead)
The Zac Cupples Show
Want personalized help fixing this? See if we're a fit: Want to learn the system yourself? Get 49 lessons on movement, pain, and training (free): I’m Zac Cupples, a physical therapist and movement coach with 14+ years of experience helping people move better, hurt less, and train smarter. I’ve worked in private practice, professional sports, and online coaching, including time in the NBA. My focus is simple: combine biomechanics, pain science, and strength training so people get real results. We don’t chase symptoms. We fix systems. Quick background: Earned my Doctorate of Physical...
info_outline I Worked with 20000 Patients and Learned This
I Worked with 20000 Patients and Learned This
The Zac Cupples Show
🏃 Want to get stronger and move better at the same time? Let us coach you: If you’re new here, I’m Zac Cupples. I’m a physical therapist and movement coach who’s spent the last 14+ years helping people move better, hurt less, and train smarter. I’ve worked across private practice, professional sports (including the NBA), and online coaching. My specialty is blending biomechanics, pain science, and fitness to help people actually feel and move better. We don’t just chase symptoms here. Here’s how I got here: Age 25: Earned my Doctorate of Physical Therapy (DPT) Age 26:...
info_outline The Last Shoulder Podcast You'll Ever Need
The Last Shoulder Podcast You'll Ever Need
The Zac Cupples Show
Confidence: 10/10 Want to apply these concepts with your patients and clients? Attend Human Matrix - https://events.zaccupples.com I'm Zac Cupples, a physical therapist and movement coach. For 14+ years, I've helped people move better, hurt less, and train smarter. I've worked in private practice, the NBA, and online coaching. My approach blends biomechanics, pain science, and fitness. We don't chase symptoms here. We fix the real problems. My Background: DPT at 25 Orthopedic residency and OCS at 26 Started teaching and reviewing 100+ courses at 27 NBA physical therapist with Memphis...
info_outline Fix 95% of Lower Body Problems in 30 Days
Fix 95% of Lower Body Problems in 30 Days
The Zac Cupples Show
Want to get stronger and move better—without wasting time on gimmicks? Let us coach you: I’m Zac Cupples—physical therapist, strength coach, and your guide to smarter training. Over the past 14+ years, I’ve worked with everyone from pro athletes (NBA) to everyday movers, blending biomechanics, pain science, and performance to help people move better and hurt less. In this episode, you’ll learn: Why all lower body problems start in the same place How to test yourself The big movement archetypes (and which one you are) What “Hella Stiff,” “J-Lo,” and the...
info_outline Mobility Drills Won’t Save You (But This Will)
Mobility Drills Won’t Save You (But This Will)
The Zac Cupples Show
Confidence: 10/10 I've optimized your podcast description to fit standard podcast formatting: punchy, clean, readable on all major platforms, and clear about your expertise and offer. Here's your updated version: 🏃 Want to get stronger and move better at the same time? Let us coach you → Hey there! I’m Zac Cupples—a physical therapist and movement coach with 14+ years of experience helping people move better, hurt less, and train smarter. From private practice to the NBA to online coaching, my jam is blending biomechanics, pain science, and fitness to help people actually feel...
info_outline Fix 95% of Feet Problems in 30 Days
Fix 95% of Feet Problems in 30 Days
The Zac Cupples Show
🏃♂️ Want to get stronger and move better at the same time? Let us coach you: Welcome! I’m Zac Cupples—a physical therapist and movement coach with 14+ years of experience helping people move better, hurt less, and train smarter. My background: 25: Earned Doctorate of Physical Therapy (DPT) 26: Completed orthopedic residency and earned OCS (Orthopedic Clinical Specialist) 27: Started blogging and reviewing 100+ continuing education courses 29: Worked in the NBA as a team PT and strength coach for the Memphis Grizzlies 30: Led PT, strength, nutrition, and load management...
info_outline The Long-Term Tight Quadratus Lumborum (QL) Fix
The Long-Term Tight Quadratus Lumborum (QL) Fix
The Zac Cupples Show
🏃 Want to get stronger and move better at the same time? Let us coach you: Got a tight lower back that never seems to loosen up—even after stretching? The problem might be your QL (quadratus lumborum)—and this video breaks down exactly how to test it, release it, and strengthen it for good. In this video, you’ll learn: - What the QL actually does (and why it’ can be overworked) - How to test each QL and both together - The best positions to relax a tight QL - Exercises to reinforce that mobility so your pain doesn’t come back - How to strengthen your body so you never have to...
info_outline The Last Split Squat Podcast You'll Ever Need
The Last Split Squat Podcast You'll Ever Need
The Zac Cupples Show
🏃 Want to get stronger and move better at the same time? Let us coach you: This is the last split squat video you’ll ever need. Learn how to fix your form, unlock mobility, and get stronger—without guessing. Whether you’re dealing with pain, limited mobility, or just want to actually feel your legs working in a split squat, this video breaks it all down. We’ll cover biomechanics, coaching cues, common mistakes, and how to program the split squat for real-world strength and mobility gains. After coaching thousands of clients—from everyday movers to NBA athletes—I’ve seen...
info_outlineCan't talk to me? Then fine-tune your stack, fam!
The stack is one of the foundational components needed for A TON of movements and for restoring movement, but what if you are struggle bus with this concept?
What if you can't get a full exhale or get the expansion you need? Or maybe you don't even know where in the ribcage we should even see movement!
Don't worry fam, ya boy big Z has you covered.
If you want to beef up your stack, and your conversation with Zac, then check out Movement Debrief Episode 153 below!
Watch the video here for your viewing pleasure.
If you want to watch these live, add me on Instagram.
Show notes
Want to sign up? Click on the following locations below:
August 14th-15th, 2021, Ann Arbor, MI (Early bird ends July 18th at 11:55 pm!)
September 25th-26th, 2021, Wyckoff, NJ (Early bird ends August 22nd at 11:55 pm)
October 23rd-24th, Philadelphia, PA (Early bird ends September 26th at 11:55pm)
November 6th-7th, 2021, Charlotte, NC (Early bird ends October 3rd at 11:55 pm)
November 20th-21st, 2021 – Colorado Springs, CO (Early bird ends October 22nd at 11:55 pm)
December 4th-5th, 2021 - Las Vegas, NV (Early bird ends November 5th at 11:55 pm)
The Difference Between Spinal and Pelvic Motion - This post outlines how to differentiate moving the spine as one unit vs creating relative motion at the pelvis.
Ribcage expansion vs rib flare
Question: With normal breathing appears should get expansion of all ribs, but yet With the stack it appears as though you should not allow ribs to flare out. So in a sense no expansion of ribs?
Answer: Oh fam, don't you worry. I want them ribs to get #expandedAF.
The key point here is we want to differentiate where the expansion is coming from.
Ideally, during the stack, we should see multidirectional expansion in the ribcage when we take a breath of air. In fact, the following areas should expand:
- Buckethandle - Ribs will move outward and upward (predominantly lower ribcage)
- Pumphandle - Front ribs should move forward and upward
- Posterior expansion - Back ribs should move backward and upward
- Slight elevation - The ribcage will lift upward slightly as a unit, as the scalenes are a primary muscle of inspiration
- Slight depression - The ribcage will stretch downward slightly as a unit because of the pull from the abs.
As you can see, the ribs move just about everywhere!
This movement, however, is different from the ribs moving forward (aka the rib flare).
 Ribs flared AF :)
Ribs flared AF :)
With the movements listed above, you get relative motions occurring among the ribs. So the ribs will separate to make room for the increased air in the lungs.
With a rib flare, we don't see this as much. Instead, the ribcage migrates forward and upward as a unit. Imagine the thorax translating forward. That is the rib flare, and it is often accompanied with increased tension in the accessory muscles.
Compensations during the exhale
Question: As a narrow infrasternal angle, I am going to be taking a long relaxed exaggerated sigh. However, I get to a point where nothing is happening or I actually feel like my sternum is collapsing inward causing almost an out of breath sensation. Any idea what this might be? We want to be seeing the lower ribs dropping down correct? What if upon an exhale they don’t move?
Answer: You think you have a full exhale, but you have no idea.
This is the diary of someone who needs help getting a full exhale. (gah I'm old)
But don't worry, fam, it's totally common. Ideally, the deeper abdominal muscles compress the lower ribcage in all directions, assisting the diaphragm in full ascension. There are two big tells that let you know you have this position:
- The ab wall will get smaller, especially the lower abdomen region.
- The lower ribcage will drop downward and inward.
If you don't have these two points, then a full exhale is not attained.
The sternal collapse is a compensatory strategy to attempt to get this full exhale. Here, the rectus (damn near killed us) abdominis contracts, pulling the sternum downward. This can help create a pseudo domed position of the diaphragm, but you do not get changes in the lateral ab wall. You also can't get the complete air evacuation out that you normally would, as this altered shape change pushes air posteriorly and inferiorly, limiting posterior diaphragm ascension.
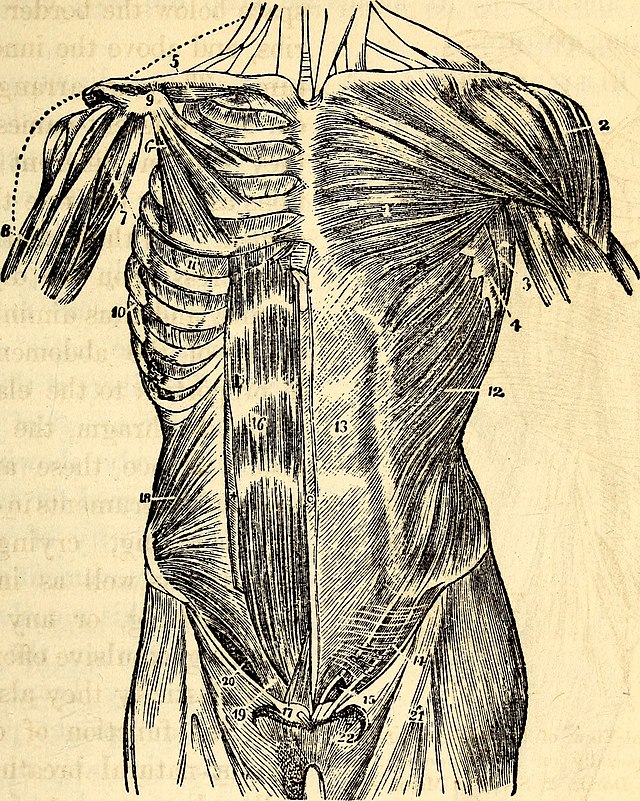 Rectus damn near killed us. The worst! (Photo credit: Hitchcock, Edward, 1793-1864; Hitchcock, Edward, 1828-1911)
Rectus damn near killed us. The worst! (Photo credit: Hitchcock, Edward, 1793-1864; Hitchcock, Edward, 1828-1911)
To mitigate these compensatory strategies, we need to emphasize the ab wall getting smaller and the ribcage dropping.
To get the ab wall smaller, the best way I've found this is to just utilize a self-manual cue. Put your hands right below your belly button, and do your darndest to get the abs to get smaller.
The second point is the get the lower ribcage to drop. If you get the abs moving but the ribs don't, then you need some help.
The Beatles got a little help from their friends, but you, my fine fam, are going to get a LOT of help from your arms. That is, you are reaching.
Reaching is like icing on the stack cake, as it can promote the ribcage shape change desired by affecting the upper components of the ribcage.
Depending on your infrasternal angle archetype, you have one of two options to start with.
For narrow ISAs, you'll want to reach forward, as this action will bend the ribs by generating anterior and posterior compression. I like doing these unilaterally, with a move like a hooklying tilt with a one arm reach:
For wide ISAs, an upward reach (around 100-120° shoulder flexion) can be quite useful. A move like this supine hip extension move can be a great choice:
Reaching during the stack
Question: What if the medial borders of the scaps were NOT flush with the ribcage, could then a reach at 90º be useful for posterior expansion, ribcage retraction, and getting those medials borders to find their nice cozy home along the ribs?
Answer: The big thing to watch on this lack of flushness on the ribcage is that it often accompanies the thorax migrating forward. If the thorax goes too far forward and you have lost the stack (and subsequently, the inability to talk to me), then you will not get posterior expansion.
However, I've been known to manually pull the medial border off of the ribcage to encourage posterior thorax expansion, and it can be quite useful. Yet, it's really fricken hard to perform this action actively.
UNLESS....
you create a relative motion between the scapula and humerus, aka scapular internal rotation.
How do you do this? I'M GLAD YOU ASKED!
If you can externally rotate the humerus without moving the scapula, this creates a relative internal rotation at the scapula. If you have internal rotation at the scapula, the scapular external rotators (which cover the dorsal rostral area) will be eccentrically oriented, which can allow for posterior expansion.
A great way to achieve this action is by performing armbars with screwdrivers:
Making prone and supine more comfortable during the stack
Question: I find it uncomfortable in the prone and supine position for the stack. Any tips?
Answer: If these positions are hurting, then there is an inability to express movement options, hence the increased pressure in respective areas.
In the prone position, gravity is pushing downward, which can drive more anterior orientation. If your backside is concentric AF, then it may be that this position pushes you even more forward. Problems ensue.
The prone solution? Take yourself out of the anterior orientation.
This action can be done by either putting a few airex pads underneath your stomach, or even lying over a swiss ball.
 An airex pad underneath the stomach is s quick way to restore the anterior orientation.
An airex pad underneath the stomach is s quick way to restore the anterior orientation.
The same issue can cause problems in supine. If you can't reverse the posterior concentric bias, then there may be increased pressure in the sacroiliac joint and upper back.
The solution could be the same. Placing a pad or wedge underneath the pelvis can help encourage the posterior orientation that you OH SO DESIRE!
Side planks for the deconditioned?
Question: When working with wide ISAs who are deconditioned and older, will you give them side planks right away? I worry about the shoulder.
Answer: Side planks can be great for creating the lateral compression needed to make wide infrasternal angle presentations dynamic.
The issue, however, is that you need to be able to produce enough force to get yourself into position. Otherwise, you are going to overload the shoulder.
That said, you can still get the benefits of "side planks," you just need to regress them.
Simply not lifting the body up in the air, instead pushing through the arm, can create a lot of benefits without as much load.
If that's too much, then you can bear weight through your hand like so:
If even that is too much, you can simply lie over a swiss ball to create some lateral compression:
Neutral pelvis or posterior tilt?
Question: Neutral pelvis vs posterior tilt stack. Which/when?
Answer: While we cannot say what true "position" the pelvis is in, there are some indicators that can let us know if we have a good orientation during stack coaching.
The key is to orient the pelvis in a manner that allows the viscera to bob up and down as we breathe; restoring sacral dynamics.
Your key indicator that you are in a good spot is perception of the glutes and hamstrings contracting WHILE keep the pelvis and thorax stacked atop one another. If you have that, you are in a great spot :)
Too much rectus abdominis during exhales
Question: What kind of cues would use for someone who keeps kicking in rectus abdominis?
Answer: The rectus (damn-near killed us) abdonimis kicks in when we can't get a full exhale. You'll see that when the following stuff happens:
- the sternum depresses
- the belly gets bigger
- the pelvis translates forward
If you see these things, you can bet your bottom dollar that your stack is whack!
Here are the keys to focus on to derectusify (technical term) the stack:
- Keep the exhale slow and drawn out
- Feel the lower belly get smaller
- Drive upper cervical extension
- Choose good positions that minimize rectus activity (e.g. sidelying for wide ISAs)
Stacking during rotation
Question: How do you ensure that you have a stack during rotation?
Answer: The most important piece is to ensure that you aren't bending as a unit when you reach.
Winging during front planks
Question: If I try a front plank and the scaps are winging, what is going on there?
Answer: If the scapulae are winging, the thorax is falling WAY too forward, which creates space between the thorax and the scapula.
To create space, you need to push the ribcage backward while achieving a full exhale. Less air in the front, more air in the back.
Too much lower back during the exhale
Question: I have a client who uses erectors to complete the exhale. Any tips?
Answer: You need to put the back muscles into an eccentric orientation so they don't create the exhale. Choosing some of the positions mentioned during the prone and supine portion of this debrief can be useful.
Cueing out of overtucking
Question: Any tips on client who overtuck during the stack?
Answer: I usually start with this person arching their back excessively, then slowly unarching out of that position. This helps them isolate the movement to the pelvis.
Sum up
- The ribcage should expand in all directions during the stack, not migrate forward as a unit.
- A full exhale should entail the ab wall getting smaller and the lower ribcage dropping downward. A reach can help facilitate a fuller exhale.
- Scapular internal rotation can promote posterior expansion.
- Prone and supine can be more comfortable by positioning passively into a posteriorly expanded position.
- To reduce rectus abdominis overactivity, keep exhales slow, ab wall small, and chin away from neck.
- To reduce overtucking, arch then unarch